

Anterior cruciate ligament (ACL) injuries are amongst the most common type of injuries affecting today’s athletes. According to the Canadian Academy of Sport and Exercise Medicine, about 250,000 ACL injuries occur in the USA and Canada each year. ACL injuries are usually caused by either an impact or a sudden shift in knee position; according to the American Academy of Orthopedic Surgeons, 70 percent of ACL injuries in athletes happen through sudden movements, like pivoting, cutting, sidestepping, out of control play or awkward landings, while about 30 percent of ACL injuries occur from contact with other players.
Epidemiology: More prevalent in active young people or during playing sports. Female>male
Short-term impact: disability, decreased physical activity, knee instability, disruption of lifestyle (work, school, family activities)
Long-term impact: increased prevalence of Knee osteoarthritis after 10 – 15 years – either surgical or non-surgical route
Young athletes: loss of athlete identity, university disruption, depression
Mechanism of Injury: 4 theories
1 – Ligament dominance: suggest that cutting maneuvers, sports requiring landing or jumping movements – produces a combo of: Knee valgus + Hip Adduction + internal rotation = ACL injury
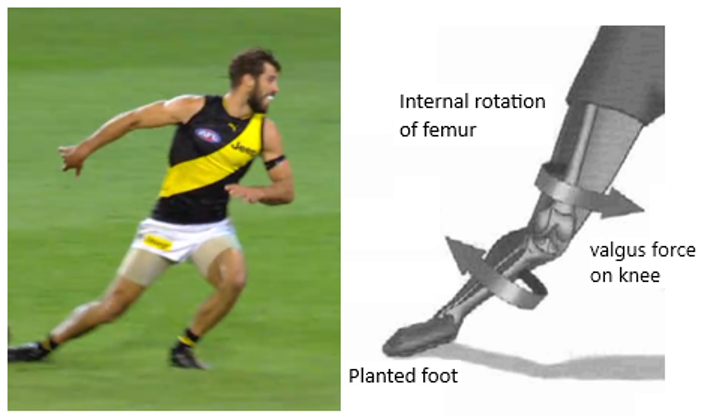
Picture 1: Most common MOI
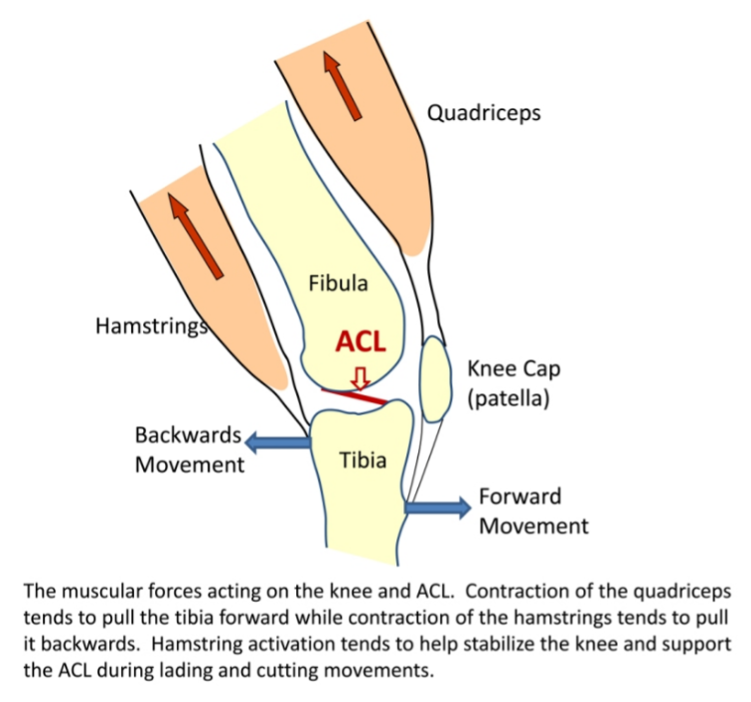
2- Quadriceps dominance: muscle strength imbalance: Quadriceps versus hamstrings – increases anterior translation of the tibia – more frequently seen in women
Source: https://symmetryptmiami.com/acl-injury-movement-patterns/
3 – Trunk dominance: uncontrolled trunk movements (heaviest body mass) + cutting maneuvers, sports requiring landing or jumping movements – increases load on the knee

Source: Hub-health
4 – Leg dominance: overuse of the same side or sports biomechanics
Prevention
Strategy: combo of trunk + Hip + knee dynamic control
IRRP: Injury Risk Reduction Programs – focus on:
- better leg alignment
- faster floor reaction time
- sport specific movement – biomechanics and overuse
- sex specific: wider pelvis = increased knee valgus = women present higher risk for sprains
- PROTECTIVE: good trunk/hip/leg neuromuscular balance
NON-SURGICAL X SURGICAL TREATMENT
Non-Surgical
- possibility of natural healing reported by studies + physiotherapy and exercise training
- NEW studies: still lacking evidence – strict bracing protocols to allow healing for 6/8 weeks + physiotherapy + exercise training
- pathway most taken for sprains grade 1 and 2 – Great outcomes!
- Great outcomes with strengthening program – restores dynamic stability and confidence
- persisting symptoms (pain, swelling, reduced knee range of motion, unstable joint) – no significantly better outcomes compared to surgical approach
- some people choose to have surgery after failing non-surgical approach
Surgical
- may have better outcomes on the long run
- no significantly better outcomes in terms of pain levels
- professional athletes – medical team + client + carrier decision (Oilers captain Connor Mc David is an example of a high-end hockey player that decided to follow a non-surgical route for a knee injury, after 2 orthopaedic surgeons referred him for a knee surgery. A combo of physiotherapy, exercise training and other therapies allowed him to go back safely to play at high levels 🙂 )
- candidates chosen based on multiple factors such as: sports specificity, personality traits, mental/financial/lifestyle status
- muscle strength-deficits: may persists overtime and are donor-site specific (patellar or hamstring tendon)
- the younger the higher the likelihood of re-injury – Males > females
- timeline to go back safely to sports activities after the surgery: at least 9 to 12 months
- higher risk of infection
- restores laxity/stability of ligament surgically
Physiotherapy after ACL tear
The general goals of rehabilitating an injured ACL are as follows:
Education
- Do’s and Dont’s
- Long term consequences: increased risk for knee Osteoarthritis
- Increased risk for re-injury
- Alternative sports
Activity modification
- rehab journey milestones: (regain full knee ROM, improve function, improve muscle strength, balance, biomechanics symmetry, dynamic stability, reaction time, neuromuscular control with dynamic activities and decrease re-injury risk)
- sports specific drills training
- objective return to sports criteria – based on above milestones achievement
What to expect if I decide to have surgery?
Acute Stage
In this stage of the injury, whether surgery is being considered or not, physiotherapy focuses on reducing inflammation and pain and regaining functional range of motion (ROM), strength, and knee stability.
In order to reduce swelling and inflammation, PRICE principles are followed: Protect, Rest, Ice, Compress and Elevate. Modalities such as ultrasound and interferential current (IFC) may also help reduce pain and swelling in the knee. In order to maintain stability and protect the knee at this stage, taping and/or bracing are used.
ROM exercises include simple flexion/extension movements of the knee to the tolerable range limited by pain, and gentle movements (such as slow kicks and cycling motions). Strengthening should focus on either isometric or closed kinetic chain for extension (straightening the knee) motions to avoid further injury to the ACL. These include straight leg raises and pushing the back of the knee down onto the bed with the knee straight. Strengthening knee flexion (bending of the knee) may be done with one lying on the tummy and bending the knee in that position.
Before the Surgery
Preparation for surgery is a stage that builds upon the acute stage protocols. These include continuing to reduce the pain and inflammation of the knee and progressing exercises that were initially introduced to continue improving range of motion and strength in the knee. One should gain the most function as possible before the surgery in order to speed up the recovery time. Prior to surgery, the knee should have little to no swelling, a full range of motion and a normal (or close to normal) gait pattern.
In this stage, mental preparation for the surgery is also enforced, including education on what to expect after the surgery and the recovery process. Strategies to help manage the immediate post-surgery phase, such as how to use crutches and how to go up and downstairs with them, are also introduced.

Post-Surgery
Different surgeons have different protocols as to how to progress exercises and load-bearing after surgery. The following is one of the protocols on the recovery process after surgery:
Week 1:
RICE principles are applied to reduce swelling and inflammation. Braces and crutches are mandatory at this stage. The goal of the first week is to achieve full extension and 70 degrees of flexion. Strengthening exercises for the quadriceps, hamstrings, and gastrocnemius (calf) muscles are also given.
Week 3-4:
With improving strength and range, progression in crutch usage occurs – first learning to use just one crutch. Strengthening exercises continues to focus on closed-kinetic chain and isometric exercises. A stationary bike is often used to help improve knee range of motion, with the goal of being able to complete one rotation (requires at least 90 degrees of knee flexion).
Week 5:
Progression of exercises continues based on how much pain and swelling is in the knee. At this stage, the usage of the knee brace is gradually reduced. Balance and proprioception exercises may begin if strength is good and pain is sufficiently reduced. More complex and intensive strengthening exercises may begin.
Week 10:
Dynamic exercises, such as backward and lateral movements are introduced. Isokinetic training, such as riding a stationary bike and walking on treadmills may begin in earnest.
Month 3:
Functional exercises such as running and jumping are introduced at 3 months. Work on agility, proprioception, and balance continue.
Month 4-5 and Beyond:
For return to full function to occur, one needs to continue improving knee endurance, and strengthen the knee stabilizers. Functional drills, some of which may be sports specific, may be introduced. These could include specific footwork techniques, sudden acceleration/deceleration drills and running and cutting maneuvers. Follow up visits with the physiotherapist should occur regularly in order to continue progressing the exercises until the athlete is at full function.
Contact one of our physiotherapists at Vansports Physio if you have any additional questions on how to recover from an ACL injury!
Source:
- Campbell et al. Canadian Academy of Sport and Exercise Medicine Position
Statement: Neuromuscular Training Programs Can Decrease Anterior Cruciate Ligament Injuries in Youth Soccer Players. Clin J Sport Med 2014;24:263–267
- Woo, S. et al. Biomechanics of Knee Ligaments. The American Journal of Sports Medicine 1999;27:533
- S. van Grinsven, R. E. H. van Cingel, C. J. M. Holla, C. J. M. van Loon. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2010; 18:1128–1144